Mycosis Fungoides (Including Sézary Syndrome) Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Mycosis Fungoides (Including Sézary Syndrome)
Mycosis fungoides and Sézary syndrome are diseases in which lymphocytes (a type of white blood cell) become malignant (cancerous) and affect the skin.
Normally, the bone marrow makes blood stem cells (immature cells) that become mature blood stem cells over time. A blood stem cell may become a myeloid stem cell or a lymphoid stem cell. A myeloid stem cell becomes a red blood cell, white blood cell, or platelet. A lymphoid stem cell becomes a lymphoblast and then one of three types of lymphocytes (white blood cells):
- B-cell lymphocytes that make antibodies to help fight infection.
- T-cell lymphocytes that help B-lymphocytes make the antibodies that help fight infection.
- Natural killer cells that attack cancer cells and viruses.
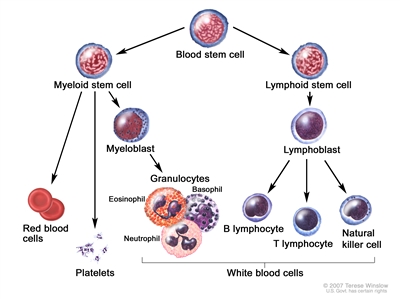
Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
In mycosis fungoides, T-cell lymphocytes become cancerous and affect the skin. When these lymphocytes occur in the blood, they are called Sézary cells. In Sézary syndrome, cancerous T-cell lymphocytes affect the skin and large numbers of Sézary cells are found in the blood.
Mycosis fungoides and Sézary syndrome are types of cutaneous T-cell lymphoma.
Mycosis fungoides and Sézary syndrome are the two most common types of cutaneous T-cell lymphoma (a type of non-Hodgkin lymphoma). For information about other types of skin cancer or non-Hodgkin lymphoma, see the following PDQ summaries:
- Adult Non-Hodgkin Lymphoma Treatment
- Skin Cancer Treatment
- Melanoma Treatment
- Kaposi Sarcoma Treatment
A sign of mycosis fungoides is a red rash on the skin.
Mycosis fungoides may go through the following phases:
- Premycotic phase: A scaly, red rash in areas of the body that usually are not exposed to the sun. This rash does not cause symptoms and may last for months or years. It is hard to diagnose the rash as mycosis fungoides during this phase.
- Patch phase: Thin, reddened, eczema -like rash.
- Plaque phase: Small raised bumps (papules) or hardened lesions on the skin, which may be reddened.
- Tumor phase: Tumors form on the skin. These tumors may develop ulcers and the skin may get infected.
Check with your doctor if you have any of these signs.
In Sézary syndrome, cancerous T-cells are found in the blood.
Also, skin all over the body is reddened, itchy, peeling, and painful. There may also be patches, plaques, or tumors on the skin. It is not known if Sézary syndrome is an advanced form of mycosis fungoides or a separate disease.
Tests that examine the skin and blood are used to diagnose mycosis fungoides and Sézary syndrome.
The following tests and procedures may be used:
- Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps, the number and type of skin lesions, or anything else that seems unusual. Pictures of the skin and a history of the patient's health habits and past illnesses and treatments will also be taken.
- Complete blood count with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells and platelets.
- The number and type of white blood cells.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the blood sample made up of red blood cells.
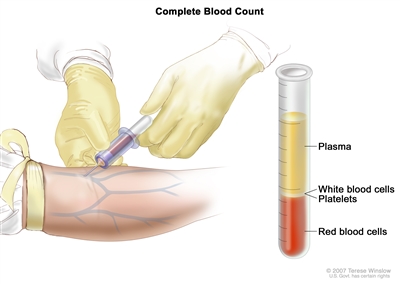
Complete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions. - Sézary blood cell count: A procedure in which a sample of blood is viewed under a microscope to count the number of Sézary cells.
- HIV test: A test to measure the level of HIV antibodies in a sample of blood. Antibodies are made by the body when it is invaded by a foreign substance. A high level of HIV antibodies may mean the body has been infected with HIV.
- Skin biopsy: The removal of cells or tissues so they can be viewed under a microscope to check for signs of cancer. The doctor may remove a growth from the skin, which will be examined by a pathologist. More than one skin biopsy may be needed to diagnose mycosis fungoides. Other tests that may be done on the cells or tissue sample include the following:
- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of lymphoma.
- Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient's blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
- T-cell receptor (TCR) gene rearrangement test: A laboratory test in which cells in a sample of blood or bone marrow are checked to see if there are certain changes in the genes that make receptors on T cells (white blood cells). Testing for these gene changes can tell whether large numbers of T cells with a certain T-cell receptor are being made.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- The stage of the cancer.
- The type of lesion (patches, plaques, or tumors).
- The patient's age and gender.
Mycosis fungoides and Sézary syndrome are hard to cure. Treatment is usually palliative, to relieve symptoms and improve the quality of life. Patients with early stage disease may live many years.
Treatment Option Overview
There are different types of treatment for patients with mycosis fungoides and Sézary syndrome cancer.
Different types of treatment are available for patients with mycosis fungoides and Sézary syndrome. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Seven types of standard treatment are used:
Photodynamic therapy
Photodynamic therapy is a cancer treatment that uses a drug and a certain type of laser light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein. The drug collects more in cancer cells than in normal cells. For skin cancer, laser light is shined onto the skin and the drug becomes active and kills the cancer cells. Photodynamic therapy causes little damage to healthy tissue. Patients undergoing photodynamic therapy will need to limit the amount of time spent in sunlight. There are different types of photodynamic therapy:
- In psoralen and ultraviolet A (PUVA) therapy, the patient receives a drug called psoralen and then ultraviolet A radiation is directed to the skin.
- In extracorporeal photopheresis (ECP), the patient is given drugs and then some blood cells are taken from the body, put under a special ultraviolet A light, and put back into the body. ECP may be used alone or combined with total skin electron beam (TSEB) radiation therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Sometimes, total skin electron beam (TSEB) radiation therapy is used to treat mycosis fungoides and Sézary syndrome. This is a type of external radiation treatment in which a radiation therapy machine aims electrons (tiny, invisible particles) at the skin covering the whole body. External radiation therapy may also be used as palliative therapy to relieve symptoms and improve quality of life.
Ultraviolet A (UVA) radiation therapy or ultraviolet B (UVB) radiation therapy may be given using a special lamp or laser that directs radiation at the skin.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). Sometimes the chemotherapy is topical (put on the skin in a cream, lotion, or ointment).
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and Sézary syndrome are types of non-Hodgkin lymphoma.)
Other drug therapy
Topical corticosteroids are used to relieve red, swollen, and inflamed skin. They are a type of steroid. Topical corticosteroids may be in a cream, lotion, or ointment.
Retinoids, such as bexarotene, are drugs related to vitamin A that can slow the growth of certain types of cancer cells. The retinoids may be taken by mouth or put on the skin.
Lenalidomide is a drug that helps the immune system kill abnormal blood cells or cancer cells and may prevent the growth of new blood vessels that tumors need to grow.
Vorinostat and romidepsin are two of the histone deacetylase (HDAC) inhibitors used to treat mycosis fungoides and Sézary syndrome. HDAC inhibitors cause a chemical change that stops tumor cells from dividing.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and Sézary syndrome are types of non-Hodgkin lymphoma.)
Immunotherapy
Immunotherapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This cancer treatment is a type of biologic therapy.
- Interferon: This treatment interferes with the division of mycosis fungoides and Sézary cells and can slow tumor growth.
See Drugs Approved for Non-Hodgkin Lymphoma for more information. (Mycosis fungoides and Sézary syndrome are types of non-Hodgkin lymphoma.)
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do.
- Monoclonal antibodies: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Types of monoclonal antibodies include:
- Brentuximab vedotin, which contains a monoclonal antibody that binds to a protein, called CD30, found on some types of lymphoma cells. It also contains an anticancer drug that may help kill cancer cells.
- Mogamulizumab, which contains a monoclonal antibody that binds to a protein, called CCR4, found on some types of lymphoma cells. It may block this protein and help the immune system kill cancer cells. It is used to treat mycosis fungoides and Sézary syndrome that came back or did not get better after treatment with at least one systemic therapy.
High-dose chemotherapy and radiation therapy with stem cell transplant
High doses of chemotherapy and sometimes radiation therapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy and radiation therapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Immune checkpoint inhibitor therapy
- Immune checkpoint inhibitor therapy: Immune checkpoint inhibitors block proteins called checkpoints that are made by some types of immune system cells, such as T cells, and some cancer cells. These checkpoints help keep immune responses from being too strong and sometimes can keep T cells from killing cancer cells. When these checkpoints are blocked, T cells can kill cancer cells better.
- PD-1 and PD-L1 inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body's immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells. Pembrolizumab is a type of PD-1 inhibitor.
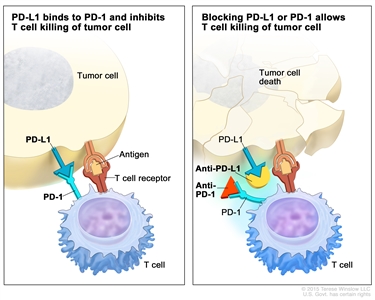
Immune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
Information about clinical trials is available from the NCI website.
Treatment for mycosis fungoides and Sézary syndrome may cause side effects.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).

