Testicular Cancer Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Testicular Cancer
Testicular cancer is a disease in which malignant (cancer) cells form in the tissues of one or both testicles.
The testicles are 2 egg-shaped glands located inside the scrotum (a sac of loose skin that lies directly below the penis). The testicles are held within the scrotum by the spermatic cord, which also contains the vas deferens and vessels and nerves of the testicles. 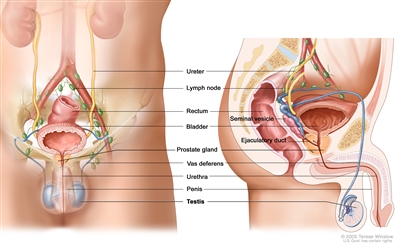
Anatomy of the male reproductive and urinary systems, showing the testicles, prostate, bladder, and other organs.
The testicles are the male sex glands and produce testosterone and sperm. Germ cells within the testicles produce immature sperm that travel through a network of tubules (tiny tubes) and larger tubes into the epididymis (a long coiled tube next to the testicles) where the sperm mature and are stored.
Almost all testicular cancers start in the germ cells. The two main types of testicular germ cell tumors are seminomas and nonseminomas. These 2 types grow and spread differently and are treated differently. Nonseminomas tend to grow and spread more quickly than seminomas. Seminomas are more sensitive to radiation. A testicular tumor that contains both seminoma and nonseminoma cells is treated as a nonseminoma.
Testicular cancer is the most common cancer in men 20 to 35 years old.
Health history can affect the risk of testicular cancer.
Anything that increases a person's chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop testicular cancer, and it will develop in people who don't have any known risk factors. Talk with your doctor if you think you may be at risk. Risk factors for testicular cancer include:
- Having had an undescended testicle.
- Having had abnormal development of the testicles.
- Having a personal history of testicular cancer.
- Having a family history of testicular cancer (especially in a father or brother).
- Being White.
Signs and symptoms of testicular cancer include swelling or discomfort in the scrotum.
These and other signs and symptoms may be caused by testicular cancer or by other conditions. Check with your doctor if you have any of the following:
- A painless lump or swelling in either testicle.
- A change in how the testicle feels.
- A dull ache in the lower abdomen or the groin.
- A sudden build-up of fluid in the scrotum.
- Pain or discomfort in a testicle or in the scrotum.
Tests that examine the testicles and blood are used to diagnose testicular cancer.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Physical exam of the testes: An exam in which a doctor checks for lumps, swelling, or pain in the testicles.
- Ultrasound exam of the testes: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram.
- Serum tumor marker test: A procedure in which a sample of blood is examined to measure the amounts of certain substances released into the blood by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called tumor markers. The following tumor markers are used to detect testicular cancer:
- Alpha-fetoprotein (AFP).
- Beta-human chorionic gonadotropin (beta-hCG).
- Inguinal orchiectomy: A procedure to remove the entire testicle through an incision in the groin. A tissue sample from the testicle is then viewed under a microscope to check for cancer cells. (The surgeon does not cut through the scrotum into the testicle to remove a sample of tissue for biopsy, because if cancer is present, this procedure could cause it to spread into the scrotum and lymph nodes. It's important to choose a surgeon who has experience with this kind of surgery.) If cancer is found, the cell type (seminoma or nonseminoma) is determined in order to help plan treatment.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- Stage of the cancer (whether it is in or near the testicle or has spread to other places in the body, and blood levels of AFP, beta-hCG, and LDH).
- Type of cancer.
- Size of the tumor.
- Number and size of retroperitoneal lymph nodes.
Testicular cancer can usually be cured in patients who receive adjuvant chemotherapy or radiation therapy after their primary treatment.
Treatment for testicular cancer can cause infertility.
Certain treatments for testicular cancer can cause infertility that may be permanent. Patients who may wish to have children should consider sperm banking before having treatment. Sperm banking is the process of freezing sperm and storing it for later use.
Stages of Testicular Cancer
After testicular cancer has been diagnosed, tests are done to find out if cancer cells have spread within the testicles or to other parts of the body.
The process used to find out if cancer has spread within the testicles or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the abdomen, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the abdomen. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Abdominal lymph node dissection: A surgical procedure in which lymph nodes in the abdomen are removed and a sample of tissue is checked under a microscope for signs of cancer. This procedure is also called lymphadenectomy. For patients with nonseminoma, removing the lymph nodes may help stop the spread of disease. Cancer cells in the lymph nodes of seminoma patients can be treated with radiation therapy.
- Serum tumor marker test: A procedure in which a sample of blood is examined to measure the amounts of certain substances released into the blood by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called tumor markers. The following 3 tumor markers are used in staging testicular cancer:
- Alpha-fetoprotein (AFP)
- Beta-human chorionic gonadotropin (beta-hCG).
- Lactate dehydrogenase (LDH).
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if testicular cancer spreads to the lung, the cancer cells in the lung are actually testicular cancer cells. The disease is metastatic testicular cancer, not lung cancer.
The following stages are used for testicular cancer:
Stage 0
In stage 0, abnormal cells are found in the tiny tubules where the sperm cells begin to develop. These abnormal cells may become cancer and spread into nearby normal tissue. All tumor marker levels are normal. Stage 0 is also called germ cell neoplasia in situ.
Stage I
In stage I, cancer has formed. Stage I is divided into stages IA, IB, and IS.
- In stage IA, cancer is found in the testicle, including the rete testis, but has not spread to the blood vessels or lymph vessels in the testicle.
All tumor marker levels are normal.
- In stage IB, cancer:
- is found in the testicle, including the rete testis, and has spread to the blood vessels or lymph vessels in the testicle; or
- has spread into the hilar soft tissue (tissue made of fibers and fat with blood vessels and lymph vessels), the epididymis, or the outer membranes around the testicle; or
- has spread to the spermatic cord; or
- has spread to the scrotum.
All tumor marker levels are normal.
- In stage IS, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum.
Tumor marker levels range from slightly above normal to high.
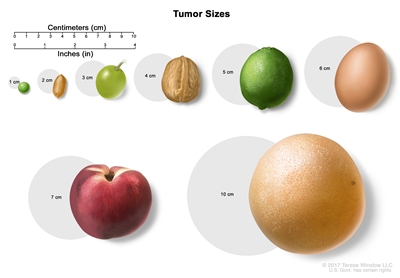
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage II
Stage II is divided into stages IIA, IIB, and IIC.
- In stage IIA, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has spread to 1 to 5 nearby lymph nodes and the lymph nodes are 2 centimeters or smaller.
All tumor marker levels are normal or slightly above normal.
- In stage IIB, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has spread to:
- 1 nearby lymph node and the lymph node is larger than 2 centimeters but not larger than 5 centimeters; or
- more than 5 nearby lymph nodes and the lymph nodes are not larger than 5 centimeters; or
- a nearby lymph node and the cancer has spread outside the lymph node.
All tumor marker levels are normal or slightly above normal.
- In stage IIC, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has spread to a nearby lymph node and the lymph node is larger than 5 centimeters.
All tumor marker levels are normal or slightly above normal.
Stage III
Stage III is divided into stages IIIA, IIIB, and IIIC.
- In stage IIIA, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer may have spread to one or more nearby lymph nodes. Cancer has spread to distant lymph nodes or to the lungs.
All tumor marker levels are normal or slightly above normal.
- In stage IIIB, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has spread:
- to one or more nearby lymph nodes and has not spread to other parts of the body; or
- to one or more nearby lymph nodes. Cancer has spread to distant lymph nodes or to the lungs.
The level of one or more tumor markers is moderately above normal.
- In stage IIIC, cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has spread:
- to one or more nearby lymph nodes and has not spread to other parts of the body; or
- to one or more nearby lymph nodes. Cancer has spread to distant lymph nodes or to the lungs.
The level of one or more tumor markers is high.
or
Cancer is found anywhere in the testicle and may have spread into the spermatic cord or scrotum. Cancer has not spread to distant lymph nodes or the lung, but has spread to other parts of the body, such as the liver or bone.
Tumor marker levels may range from normal to high.
Testicular cancer can recur (come back) after it has been treated.
The cancer may come back many years after the initial cancer, in the other testicle or in other parts of the body.
Treatment Option Overview
There are different types of treatment for patients with testicular cancer.
Different types of treatments are available for patients with testicular cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Testicular tumors are divided into 3 groups, based on how well the tumors are expected to respond to treatment.
Good Prognosis
For nonseminoma, all of the following must be true:
- The tumor is found only in the testicle or in the retroperitoneum (area outside or behind the abdominal wall); and
- The tumor has not spread to organs other than the lungs; and
- The levels of all the tumor markers are slightly above normal.
For seminoma, all of the following must be true:
- The tumor has not spread to organs other than the lungs; and
- The level of alpha-fetoprotein (AFP) is normal. Beta-human chorionic gonadotropin (beta-hCG) and lactate dehydrogenase (LDH) may be at any level.
Intermediate Prognosis
For nonseminoma, all of the following must be true:
- The tumor is found in one testicle only or in the retroperitoneum (area outside or behind the abdominal wall); and
- The tumor has not spread to organs other than the lungs; and
- The level of any one of the tumor markers is more than slightly above normal.
For seminoma, all of the following must be true:
- The tumor has spread to organs other than the lungs; and
- The level of AFP is normal. Beta-hCG and LDH may be at any level.
Poor Prognosis
For nonseminoma, at least one of the following must be true:
- The tumor is in the center of the chest between the lungs; or
- The tumor has spread to organs other than the lungs; or
- The level of any one of the tumor markers is high.
There is no poor prognosis grouping for seminoma testicular tumors.
The following types of treatment are used:
Surgery
Surgery to remove the testicle (inguinal orchiectomy) and some of the lymph nodes may be done at diagnosis and staging. (See the General Information and Stages sections of this summary.) Tumors that have spread to other places in the body may be partly or entirely removed by surgery.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
See Drugs Approved for Testicular Cancer for more information.
Surveillance
Surveillance is closely following a patient's condition without giving any treatment unless there are changes in test results. It is used to find early signs that the cancer has recurred (come back). In surveillance, patients are given certain exams and tests on a regular schedule.
High-dose chemotherapy with stem cell transplant
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood -forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
See Drugs Approved for Testicular Cancer for more information.
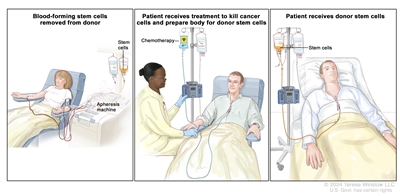
Donor stem cell transplant. (Step 1): Four to five days before donor stem cell collection, the donor receives a medicine to increase the number of stem cells circulating through their bloodstream (not shown). The blood-forming stem cells are then collected from the donor through a large vein in their arm. The blood flows through an apheresis machine that removes the stem cells. The rest of the blood is returned to the donor through a vein in their other arm. (Step 2): The patient receives chemotherapy to kill cancer cells and prepare their body for the donor stem cells. The patient may also receive radiation therapy (not shown). (Step 3): The patient receives an infusion of the donor stem cells.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for testicular cancer may cause side effects.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Men who have had testicular cancer have an increased risk of developing cancer in the other testicle. A patient is advised to regularly check the other testicle and report any unusual symptoms to a doctor right away.
Long-term clinical exams are very important. The patient will probably have check-ups frequently during the first year after surgery and less often after that.

