Childhood Central Nervous System Atypical Teratoid/Rhabdoid Tumor Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Central Nervous System Atypical Teratoid / Rhabdoid Tumor
Central nervous system (CNS) atypical teratoid/rhabdoid tumor (AT/RT) is a cancer that forms in the tissues of the brain.
Central nervous system (CNS) atypical teratoid/rhabdoid tumor (AT/RT) is a very rare, fast-growing cancer that begins in the brain and spinal cord. It usually occurs in children aged 3 years and younger, although it can occur in older children and adults.
About half of these tumors form in the cerebellum or brain stem. The cerebellum is the part of the brain that controls movement, balance, and posture. The brain stem controls breathing, heart rate, and the nerves and muscles used in seeing, hearing, walking, talking, and eating. AT/RT can also begin in other parts of the brain and spinal cord.
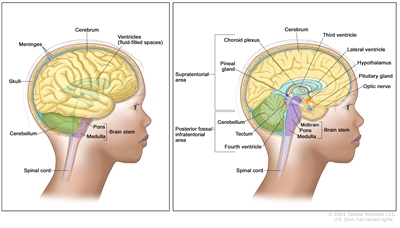
Anatomy of the brain. The supratentorial area (the upper part of the brain) contains the cerebrum, lateral ventricle and third ventricle (with cerebrospinal fluid shown in blue), choroid plexus, pineal gland, hypothalamus, pituitary gland, and optic nerve. The posterior fossa/infratentorial area (the lower back part of the brain) contains the cerebellum, tectum, fourth ventricle, and brain stem (midbrain, pons, and medulla). The skull and meninges protect the brain and spinal cord.
Certain genetic changes may increase the risk of AT/RT.
A risk factor is anything that increases the chance of getting a disease. Not every child with one or more of these risk factors will develop AT/RT. And it will develop in some children who don't have a known risk factor.
AT/RT may be linked to changes in the tumor suppressor genes SMARCB1 or SMARCA4. Tumor suppressor genes make a protein that helps control how and when cells grow. Changes in the DNA of tumor suppressor genes like SMARCB1 or SMARCA4 may lead to cancer.
The changes in the SMARCB1 or SMARCA4 genes may be inherited (passed on from parents to offspring). When this gene change is inherited, tumors may form in two parts of the body at the same time (for example, in the brain and the kidney). For children with AT/RT, genetic counseling (a discussion with a trained professional about inherited diseases and a possible need for gene testing) may be recommended.
Talk with your child's doctor if you think your child may be at risk.
The symptoms of AT/RT are not the same in every person.
Symptoms depend on:
- the child's age
- where the tumor has formed
Because AT/RT is fast growing, symptoms may develop quickly and get worse over a period of days or weeks. It's important to check with your child's doctor if your child has:
- a morning headache or headache that goes away after vomiting
- nausea and vomiting
- unusual sleepiness or change in activity level
- loss of balance, lack of coordination, or trouble walking
- an increase in head size (in infants)
- pain, tingling, numbness, or paralysis in the face
These symptoms may be caused by problems other than AT/RT. The only way to know is to see your child's doctor.
CNS AT/RT is found with tests that examine the brain and spinal cord.
If your child has symptoms that suggest AT/RT, the doctor will need to find out if these are due to cancer or another problem. The doctor will ask when the symptoms started and how often your child has been having them. They will also ask about your child's personal and family health history and do a physical exam, including a neurological exam. Depending on these results, they may recommend other tests. If your child is diagnosed with AT/RT, the results of these tests will help you and your child's doctor plan treatment.
The tests used to diagnose AT/RT may include:
- Magnetic resonance imaging (MRI) uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Lumbar puncture is a procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the lining around the spinal cord to remove a sample of the CSF. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. This procedure is also called an LP or spinal tap.
- SMARCB1 and SMARCA4 gene testing is a laboratory test in which a sample of blood or tissue is tested for certain changes in the SMARCB1 and SMARCA4 genes. Children with AT/RT may be eligible for gene testing through the Molecular Characterization Initiative.
The Molecular Characterization Initiative offers free molecular testing to children, adolescents, and young adults with certain types of newly diagnosed cancer. The program is offered through NCI's Childhood Cancer Data Initiative. To learn more, visit About the Molecular Characterization Initiative.
- Ultrasound exam uses high-energy sound waves (ultrasound) that bounce off internal tissues or organs, such as the kidney, and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is done to check for tumors that may also have formed in the kidney.
Childhood AT/RT is diagnosed using a biopsy, and the tumor may be removed in the same surgery.
If doctors think there might be a brain tumor, a biopsy may be done to remove a sample of tissue. For brain tumors, the biopsy can be done by removing part of the skull or making a small hole in the skull and using a needle or surgical device to remove a sample of tissue. Sometimes, when a needle is used, it is guided by a computer to remove the tissue sample. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. The pathologist checks the cancer cells to find out the type of brain tumor. It is often difficult to completely remove AT/RT because of where the tumor is in the brain and because it may already have spread at the time of diagnosis. The piece of skull is usually put back in place after the procedure.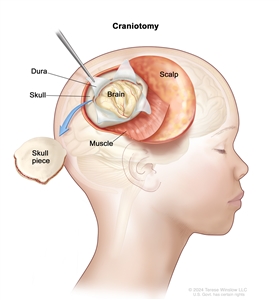
Craniotomy. An opening is made in the skull and a piece of the skull is removed to show part of the brain.
The following test may be done on the sample of tissue that is removed:
- Immunohistochemistry uses antibodies to check for certain antigens (markers) in a sample of a patient's tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
If your child has been diagnosed with AT/RT, you likely have questions about how serious the cancer is and your child's chances of survival. The likely outcome or course of a disease is called prognosis.
The prognosis depends on:
- whether your child has certain inherited gene changes
- whether the tumor has certain gene changes
- your child's age
- the amount of tumor remaining after surgery
- whether the cancer has spread to other parts of the brain and spinal cord or to the kidney at the time of diagnosis
- whether the cancer has just been diagnosed or has recurred (come back)
No two people are alike, and responses to treatment can vary greatly. Your child's cancer care team is in the best position to talk with you about your child's prognosis.
Treatment Option Overview
There are different types of treatment for children with central nervous system (CNS) atypical teratoid/rhabdoid tumor (AT/RT).
There are different types of treatment for children with AT/RT. You and your child's care team will work together to decide treatment. Many factors will be considered, such as where the cancer is located and your child's age and overall health.
Your child's treatment plan will include information about the tumor, the goals of treatment, treatment options, and the possible side effects. It will be helpful to talk with your child's care team before treatment begins about what to expect. For help every step of the way, see our booklet, Children with Cancer: A Guide for Parents.
Children with AT/RT should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
A pediatric oncologist, a doctor who specializes in treating children with cancer, oversees treatment of AT/RT. The pediatric oncologist works with other health care providers who are experts in treating children with CNS cancer and also specialize in other areas of medicine. Other specialists may include:
- pediatrician
- pediatric neurosurgeon
- radiation oncologist
- neurologist
- pediatric nurse specialist
- rehabilitation specialist
- psychologist
- social worker
- geneticist or genetic counselor
- fertility specialist
Childhood brain tumors may cause symptoms that begin before the cancer is diagnosed and continue for months or years.
Symptoms caused by the tumor may begin before diagnosis. These signs or symptoms may continue for months or years. It is important to talk with your child's doctors about symptoms caused by the tumor that may continue after treatment.
The following types of treatment may be used:
Surgery
Surgery is used to treat CNS AT/RT. Learn more about how this tumor is diagnosed.
After the doctor removes all the cancer that can be seen at the time of the surgery, most children will receive chemotherapy and possibly radiation therapy to try to kill any cancer cells that are left. Treatment given after surgery to lower the risk that the cancer will come back is called adjuvant therapy.
Chemotherapy
Chemotherapy uses drugs to stop the growth of cancer cells. Chemotherapy either kills the cells or stops them from dividing. Chemotherapy may be given with other types of treatments.
Chemotherapy for AT/RT is injected into a vein. When given this way, the drugs enter the bloodstream and can reach tumor cells throughout the body. High doses of some chemotherapy drugs given into a vein can cross the blood-brain barrier and reach the tumor. Chemotherapy for AT/RT is also placed directly into the cerebrospinal fluid (intrathecal chemotherapy). Combination chemotherapy uses more than one anticancer drug.
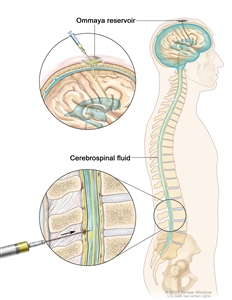
Intrathecal chemotherapy. Anticancer drugs are injected into the intrathecal space, which is the space that holds the cerebrospinal fluid (CSF, shown in blue). There are two different ways to do this. One way, shown in the top part of the figure, is to inject the drugs into an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). The other way, shown in the bottom part of the figure, is to inject the drugs directly into the CSF in the lower part of the spinal column, after a small area on the lower back is numbed.
Chemotherapy drugs used alone or in combination to treat AT/RT in children include:
- carboplatin
- cisplatin
- cyclophosphamide
- cytarabine
- etoposide
- methotrexate
- thiotepa
Other chemotherapy drugs not listed here may also be used.
Learn more about how chemotherapy works, how it is given, and common side effects at Chemotherapy to Treat Cancer.
Radiation therapy
Radiation therapy uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Because radiation therapy can affect growth and brain development in young children, especially children who are 3 years old or younger, the dose of radiation therapy may be lower than in older children.
Learn more about External Beam Radiation Therapy for Cancer and Radiation Therapy Side Effects.
Stem cell transplant
High doses of chemotherapy are given to kill cancer cells. This treatment destroys healthy cells, including blood -forming cells. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Clinical trials
For some children, joining a clinical trial may be an option. There are different types of clinical trials for childhood cancer. For example, a treatment trial tests new treatments or new ways of using current treatments. Supportive care and palliative care trials look at ways to improve quality of life, especially for those who have side effects from cancer and its treatment.
You can find clinical trials for people with atypical teratoid/rhabdoid tumor at Treatment Clinical Trials for Atypical Teratoid/Rhabdoid Tumor or use the clinical trial search to find NCI-supported cancer clinical trials accepting participants. The search allows you to filter trials based on the type of cancer, your child's age, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Learn more about clinical trials, including how to find and join one, at Clinical Trials Information for Patients and Caregivers.
Treatment for childhood CNS AT/RT may cause side effects.
Cancer treatments can cause side effects. Which side effects your child might have depends on the type of treatment they receive, the dose, and how their body reacts. Talk with your child's treatment team about which side effects to look for and ways to manage them.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Problems from cancer treatment that begin 6 months or later after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include:
- physical problems
- changes in mood, feelings, thinking, learning, or memory
- second cancers (new types of cancer)
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. Learn more about Late Effects of Treatment for Childhood Cancer.
Follow-up care may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some of the tests that were done to diagnose the cancer may be repeated. Some tests will be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back).
Resources and support are available to help you cope with your child's cancer.
When your child has cancer, every member of the family needs support. Taking care of yourself during this difficult time is important. Reach out to your child's treatment team and to people in your family and community for support. To learn more, see Support for Families: Childhood Cancer and the booklet Children with Cancer: A Guide for Parents.

