Childhood Adrenocortical Carcinoma Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Adrenocortical Carcinoma
Adrenocortical carcinoma is a rare disease in which malignant (cancer) cells form in the outer layer of the adrenal gland.
There are two adrenal glands. The adrenal glands are small and shaped like a triangle. One adrenal gland sits on top of each kidney. Each adrenal gland has two parts. The outer layer of the adrenal gland is the adrenal cortex. The center of the adrenal gland is the adrenal medulla. Adrenocortical carcinoma is also called adrenocortical cancer or cancer of the adrenal cortex.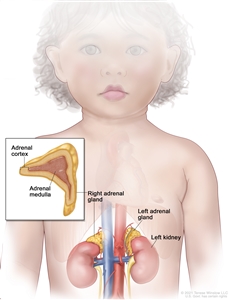
Anatomy of the adrenal gland. There are two adrenal glands, one on top of each kidney. The outer part of each gland is the adrenal cortex and the inner part is the adrenal medulla.
The adrenal cortex makes important hormones that:
- Balance the water and salt in the body.
- Help keep blood pressure normal.
- Help control the body's use of protein, fat, and carbohydrates.
- Cause the body to have male or female characteristics.
The adrenal medulla makes hormones that help the body react to stress. Cancer that forms in the adrenal medulla is called pheochromocytoma and is not discussed in this summary. See the PDQ summary on Childhood Pheochromocytoma and Paraganglioma Treatment for more information.
Most childhood adrenocortical tumors occur during the first 5 years of life, but they may also occur during adolescence.
Having a certain mutation (change) in the TP53 gene increases the risk of adrenocortical carcinoma.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your child's doctor if you think your child may be at risk.
The risk of adrenocortical carcinoma is increased by having a mutation (change) in the TP53gene or any of the following syndromes:
- Li-Fraumeni syndrome.
- Beckwith-Wiedemann syndrome.
- Hemihyperplasia.
Signs and symptoms of adrenocortical carcinoma include a lump or pain in the abdomen.
These and other signs and symptoms may be caused by adrenocortical carcinoma or by other conditions.
Check with your child's doctor if your child has any of the following:
- Pain in the abdomen or back.
- A lump in the abdomen.
- Feeling of fullness in the abdomen.
- High blood pressure.
- Acne.
- Growing body hair.
- Deepening of the voice.
- Growing faster than normal.
Also, cancer of the adrenal cortex may be functioning (makes more hormones than normal) or nonfunctioning (does not make extra hormones). Most tumors of the adrenal cortex in children are functioning tumors. The extra hormones made by functioning tumors may cause certain signs or symptoms of disease and these depend on the type of hormone made by the tumor. For example, extra androgen hormone may also cause male children to develop an enlarged penis and female children to develop enlarged genitalia. Extra estrogen hormone may cause the growth of breast tissue in male children. Extra cortisol hormone may cause (hypercortisolism).
See the PDQ summary onAdrenocortical Carcinoma Treatment (Adult) for more information on the signs and symptoms of adrenocortical carcinoma.
Tests that examine the adrenal glands are used to diagnose and stage adrenocortical carcinoma.
Tests are done to diagnose and stage cancer. After cancer is diagnosed, more tests are done to find out if cancer cells have spread to nearby areas or to other parts of the body. This process is called staging. It is important to know whether cancer has spread in order to plan the best treatment.
The following tests and procedures may be used:
- Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
- X-ray: An x-ray of the chest, abdomen, or bones inside the body. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan: A procedure that makes a series of detailed pictures of areas inside the body, such as the chest or abdomen, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
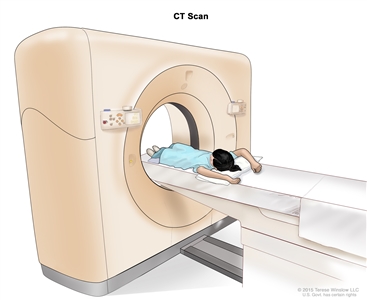
Computed tomography (CT) scan. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of areas inside the body. - MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas of the body, such as the chest and abdomen. This procedure is also called nuclear magnetic resonance imaging (NMRI).
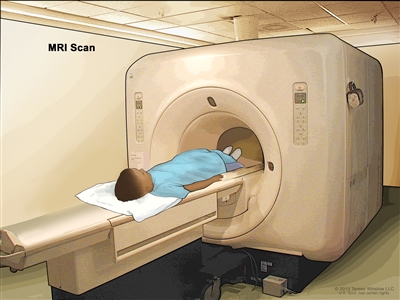
Magnetic resonance imaging (MRI) scan. The child lies on a table that slides into the MRI machine, which takes a series of detailed pictures of areas inside the body. The positioning of the child on the table depends on the part of the body being imaged. - PET scan: A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
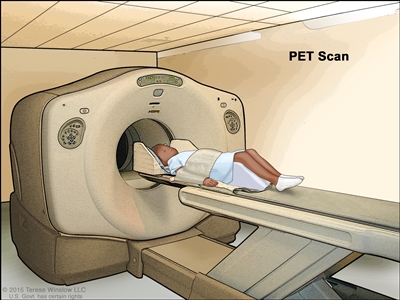
Positron emission tomography (PET) scan. The child lies on a table that slides through the PET scanner. The head rest and white strap help the child lie still. A small amount of radioactive glucose (sugar) is injected into the child's vein, and a scanner makes a picture of where the glucose is being used in the body. Cancer cells show up brighter in the picture because they take up more glucose than normal cells do. - Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs, such as the abdomen, and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
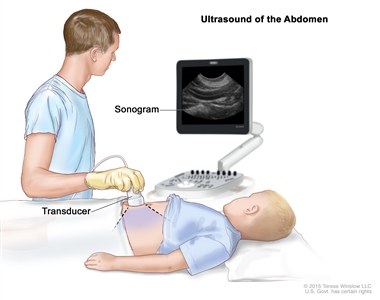
Abdominal ultrasound. An ultrasound transducer connected to a computer is pressed against the skin of the abdomen. The transducer bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture). - Biopsy: The removal of cells or tissues during surgery so they can be viewed under a microscope by a pathologist to check for signs of cancer.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Blood hormone studies: A procedure in which a blood sample is checked to measure the amounts of certain hormones released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. The blood may be checked for testosterone or estrogen. A higher than normal amount of these hormones may be a sign of adrenocortical carcinoma.
- Twenty-four-hour urine test: A test in which urine is collected for 24 hours to measure the amounts of cortisol or 17-ketosteroids. A higher than normal amount of these substances in the urine may be a sign of disease in the adrenal cortex.
- Low-dose dexamethasone suppression test: A test in which one or more small doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol.
- High-dose dexamethasone suppression test: A test in which one or more high doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol or if the pituitary gland is telling the adrenal glands to make too much cortisol.
- Adrenal angiography: A procedure to look at the arteries and the flow of blood near the adrenal gland. A contrast dye is injected into the adrenal arteries. As the dye moves through the blood vessel, a series of x-rays are taken to see if any arteries are blocked.
- Adrenal venography: A procedure to look at the adrenal veins and the flow of blood near the adrenal glands. A contrast dye is injected into an adrenal vein. As the contrast dye moves through the vein, a series of x-rays are taken to see if any veins are blocked. A catheter (very thin tube) may be inserted into the vein to take a blood sample, which is checked for abnormal hormone levels.
Certain factors affect prognosis (chance of recovery).
The prognosis is good for patients who have small tumors that have been completely removed by surgery. For other patients, the prognosis depends on the following:
- The size of the tumor.
- How quickly the cancer is growing.
- Whether there are changes in certain genes.
- Whether the tumor has spread to other parts of the body, including the lymph nodes, liver, lung, kidney, or bone.
- The child's age.
- Whether the covering around the tumor broke open during surgery to remove the tumor.
- Whether the tumor was completely removed during surgery.
- Whether the child has developed masculine traits.
Treatment Option Overview
There are different types of treatment for children with adrenocortical carcinoma.
Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Because cancer in children is rare, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not started treatment.
Children with adrenocortical carcinoma should have their treatment planned by a team of doctors who are experts in treating childhood cancer.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other pediatric health professionals who are experts in treating children with cancer and who specialize in certain areas of medicine. This may include the following specialists and others:
- Pediatrician.
- Pediatric surgeon.
- Radiation oncologist.
- Pathologist.
- Endocrinologist.
- Pediatric nurse specialist.
- Social worker.
- Rehabilitation specialist.
- Psychologist.
- Child-life specialist.
Two types of standard treatment are used:
Surgery
Surgery to remove the tumor is the main treatment for adrenocortical carcinoma.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Immunotherapy
Immunotherapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This cancer treatment is a type of biologic therapy.
- Immune checkpoint inhibitor therapy is a type of immunotherapy that blocks certain proteins. PD-1 is a protein on the surface of T cells that helps keep the body's immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells. Pembrolizumab is a PD-1 inhibitor that is being studied in the treatment of childhood adrenocortical carcinoma that is advanced or has come back after treatment.
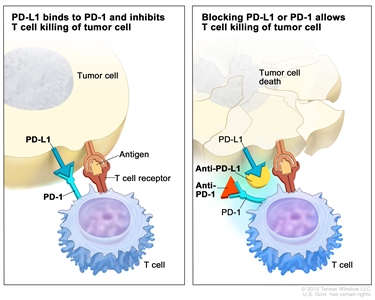
Immune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
Treatment for childhood adrenocortical carcinoma may cause side effects.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include the following:
- Physical problems, including problems with the thyroid gland, hearing, fully opening the mouth, dental cavities, and chronic sinusitis or ear infections.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer) or other conditions.
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the possible late effects caused by some treatments. See the PDQ summary on Late Effects of Treatment for Childhood Cancer. for more information.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back).

