What is screening?
Screening is looking for signs of disease, such as breast cancer, before a person has symptoms. The goal of screening tests is to find cancer at an early stage when it can be treated and may be cured. Sometimes a screening test finds cancer that is very small or very slow growing. These cancers are unlikely to cause death or illness during the person's lifetime.
Scientists are trying to better understand which people are more likely to get certain types of cancer. For example, they look at the person's age, their family history, and certain exposures during their lifetime. This information helps doctors recommend who should be screened for cancer, which screening tests should be used, and how often the tests should be done.
It is important to remember that your doctor does not necessarily think you have cancer if he or she suggests a screening test. Screening tests are done when you have no cancer symptoms. Women who have a strong family history or a personal history of cancer or other risk factors may also be offered genetic testing.
If a screening test result is abnormal, you may need to have more tests done to find out if you have cancer. These are called diagnostic tests, rather than screening tests.
For more information about cancer screening, see Cancer Screening Overview.
General Information About Breast Cancer
Breast cancer is a disease in which malignant (cancer) cells form in the tissues of the breast.
The breast is made up of lobes and ducts. Each breast has 15 to 20 sections called lobes, which have many smaller sections called lobules. Lobules end in dozens of tiny bulbs that can produce milk. The lobes, lobules, and bulbs are linked by thin tubes called ducts.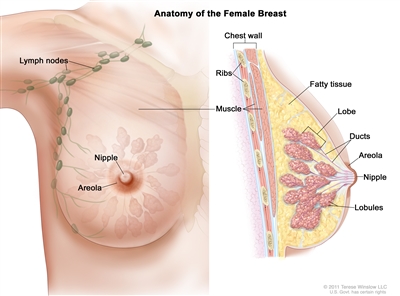
Anatomy of the female breast. The nipple and areola are shown on the outside of the breast. The lymph nodes, lobes, lobules, ducts, and other parts of the inside of the breast are also shown.
Each breast also has blood vessels and lymph vessels. The lymph vessels carry an almost colorless, watery fluid called lymph. Lymph vessels carry lymph between lymph nodes. Lymph nodes are small, bean-shaped structures that filter lymph and store white blood cells that help fight infection and disease. Groups of lymph nodes are found near the breast in the axilla (under the arm), above the collarbone, and in the chest.
For more information about breast cancer, see the following:
Breast cancer is the second leading cause of death from cancer in American women.
Women in the United States get breast cancer more than any other type of cancer except for skin cancer.
Breast cancer is more likely to occur as a woman ages. It occurs more often in White women than in Black women, but Black women die from breast cancer more often than White women.
Breast cancer rarely occurs in men. Because men with breast cancer usually have a lump that can be felt, screening tests are not likely to be helpful.
Different factors increase or decrease the risk of breast cancer.
For information about risk factors and protective factors for breast cancer, see Breast Cancer Prevention.
Breast Cancer Screening
Tests are used to screen for different types of cancer when a person does not have symptoms.
Scientists study screening tests to find those with the fewest harms and most benefits. Cancer screening trials also are meant to show whether early detection (finding cancer before it causes symptoms) helps a person live longer or decreases a person's chance of dying from the disease. For some types of cancer, the chance of recovery is better if the disease is found and treated at an early stage.
Mammography is the most common screening test for breast cancer.
A mammogram is a picture of the inside of the breast. Mammography may find tumors that are too small to feel. It may also find ductal carcinoma in situ (DCIS). In DCIS, abnormal cells line the breast duct, and in some women may become invasive cancer.
There are different types of mammograms:
- Film mammography is an x-ray picture of the breast.
- Digital mammography (DM) is a computer picture of the breast.
- Digital breast tomosynthesis (DBT) uses x-rays to take a series of pictures of the breast from many different angles. A computer is used to make 3-D pictures of the breast from these x-rays.
- 2-dimensional mammography (S2D) uses x-rays to take pictures of the inside of the breast, usually from two different angles. A computer or x-ray film is used to make 2-D pictures of the breast.
Digital breast tomosynthesis (DBT) was approved by the U.S. Food and Drug Administration (FDA) in 2018 and is now used in 3 out of 4 facilities. One recent study found that 2-dimensional mammography (S2D) combined with DBT improved tumor detection rates and lowered mammogram callbacks, radiation dose, and overall costs. More studies are being done to compare different types of breast cancer screening.
Mammography is less likely to find breast tumors in women with dense breast tissue. Because both tumors and dense breast tissue appear white on a mammogram, it can be harder to find a tumor when there is dense breast tissue. Younger women are more likely to have dense breast tissue. For more information, see Dense Breasts: Answers to Commonly Asked Questions.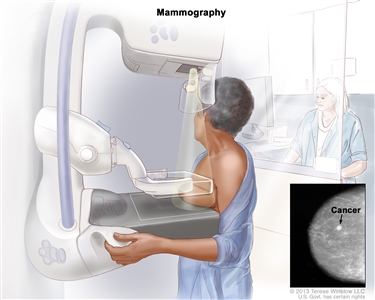
Mammography. The breast is pressed between two plates. X-rays are used to take pictures of breast tissue.
Many factors affect whether mammography is able to detect (find) breast cancer:
- The age and weight of the patient.
- The size and type of tumor.
- Where the tumor has formed in the breast.
- How sensitive the breast tissue is to hormones.
- How dense the breast tissue is.
- The timing of the mammography within the woman's menstrual cycle.
- The quality of the mammogram picture.
- The skill of the radiologist in reading the mammogram.
Women aged 50 to 69 years who have screening mammograms have a lower chance of dying from breast cancer than women who do not have screening mammograms.
Fewer women are dying of breast cancer in the United States, but it is not known whether the lower risk of dying is because the cancer was found early by screening or whether the treatments were better.
Magnetic resonance imaging (MRI) may be used to screen women who have a high risk of breast cancer.
MRI is a procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI). MRI does not use any x-rays and the woman is not exposed to radiation. 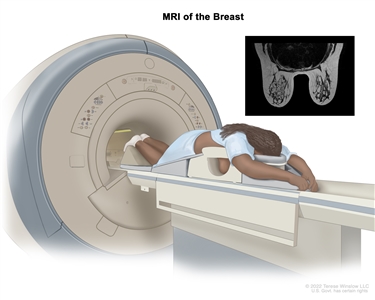
An MRI of the breast is a procedure that uses radio waves, a strong magnet, and a computer to create detailed pictures of the inside of the breast. A contrast dye may be injected into a vein (not shown) to make the breast tissues easier to see on the MRI pictures. An MRI may be used with other breast imaging tests to detect breast cancer or other abnormal changes in the breast. It may also be used to screen for breast cancer in some people who have a high risk of the disease. Note: The inset shows an MRI image of the insides of both breasts. Credit for inset: The Cancer Imaging Archive (TCIA).
MRI may be used as a screening test for women who have a high risk of breast cancer. Factors that put women at high risk include the following:
- Certain gene changes, such as changes in the BRCA1 or BRCA2 genes.
- A family history (first degree relative, such as a mother, daughter or sister) with breast cancer.
- Certain genetic syndromes, such as Li-Fraumeni or Cowden syndrome.
An MRI is more likely than mammography to find a breast mass that is not cancer.
Women with dense breasts who have supplemental screening (for example, an MRI) show higher rates of breast cancer detection, but there is limited evidence about whether this leads to better health outcomes.
Whether a woman should be screened for breast cancer and the screening test to use depends on certain factors.
Women with risk factors for breast cancer, such as certain changes in the BRCA1 or BRCA2 gene or certain genetic syndromes may be screened at a younger age and more often.
Women who have had radiation treatment to the chest, especially at a young age, may start routine breast cancer screening at an earlier age. The benefits and risks of mammograms and MRIs for these women have not been studied.
Breast cancer screening has not been shown to benefit the following women:
- Elderly women who, if diagnosed with breast cancer through screening, will usually die of other causes. Screening mammograms for those aged 66 to 79 years may find cancer in a very small percentage of women, but most of these cancers are low risk.
- In women with an average risk of developing breast cancer, screening mammography before age 40 has not shown any benefit.
- In women who are not expected to live for a long time and have other diseases or conditions, finding and treating early stage breast cancer may reduce their quality of life without helping them live longer.
Other screening tests have been or are being studied in clinical trials.
Studies have been done to find out if the following breast cancer screening tests are useful in finding breast cancer or helping women with breast cancer live longer.
Breast Exam
A clinical breast exam is an exam of the breast by a doctor or other health professional. He or she will carefully feel the breasts and under the arms for lumps or anything else that seems unusual. It is not known if having clinical breast exams decreases the chance of dying from breast cancer.
Breast self-exams may be done by women or men to check their breasts for lumps or other changes. If you feel any lumps or notice any other changes in your breasts, talk to your doctor. Doing regular breast self-exams has not been shown to decrease the chance of dying from breast cancer.
Thermography
Thermography is a procedure in which a special camera that senses heat is used to record the temperature of the skin that covers the breasts. Tumors can cause temperature changes that may show up on the thermogram.
There have been no randomized clinical trials of thermography to find out how well it detects breast cancer or the harms of the procedure.
Tissue sampling
Breast tissue sampling is taking cells from breast tissue to check under a microscope. Breast tissue sampling as a screening test has not been shown to decrease the risk of dying from breast cancer.
Screening tests for breast cancer are being studied in clinical trials.
Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Harms of Breast Cancer Screening
Screening tests can have harms.
Not all breast cancers will cause death or illness in a woman's lifetime, so they may not need to be found or treated.
Decisions about screening tests can be difficult. Not all screening tests are helpful and most have harms. Before having any screening test, you may want to discuss the test with your doctor. It is important to know the harms of the test and whether it has been proven to reduce the risk of dying from cancer.
The harms of mammography include the following:
False-positive test results can occur.
Screening test results may appear to be abnormal even though no cancer is present. A false-positive test result (one that shows there is cancer when there really isn't) is usually followed by more tests (such as biopsy), which also have risks.
When a breast biopsy result is abnormal, getting a second opinion from a different pathologist may confirm a correct breast cancer diagnosis.
Most abnormal test results turn out not to be cancer. False-positive results are more common in the following:
- Younger women (under age 50).
- Women who have had previous breast biopsies.
- Women with a family history of breast cancer.
- Women who take hormones for menopause.
False-positive results are more likely the first time screening mammography is done than with later screenings. For every ten women who have a single mammogram, one will have a false-positive result. The chance of having a false-positive result goes up the more mammograms a woman has. Comparing a current mammogram with a past mammogram lowers the risk of a false-positive result.
The skill of the radiologist also can affect the chance of a false-positive result.
False-positive results can lead to extra testing and cause anxiety.
If a mammogram is abnormal, more tests may be done to diagnose cancer. Women can become anxious during the diagnostic testing. Even if it is a false-positive test and cancer is not diagnosed, the result can lead to anxiety anywhere from a few days to years later.
Several studies show that women who feel anxiety after false-positive test results are more likely to schedule regular breast screening exams in the future.
False-negative test results can delay diagnosis and treatment.
Screening test results may appear to be normal even though breast cancer is present. This is called a false-negative test result. A woman who has a false-negative test result may delay seeking medical care even if she has symptoms. About one in 5 cancers are missed by mammography.
The chance of a false-negative test result is more common in women who:
- Are younger.
- Have dense breast tissue.
- Have cancer that is not dependent on hormones (estrogen and progesterone).
- Have cancer that is fast growing.
Finding breast cancer may lead to breast cancer treatment and side effects, but it may not improve a woman's health or help her live longer.
Some breast cancers found only by screening mammography may never cause health problems or become life-threatening. Finding these cancers is called overdiagnosis. When these cancers are found, having treatment may cause serious side effects and may not lead to a longer, healthier life.
Mammography exposes the breast to low doses of radiation.
Being exposed to high radiation doses is a risk factor for breast cancer. The radiation dose with a mammogram is very low. Women who start getting mammograms after age 50 have very little risk that the overall exposure to radiation from mammograms throughout their lives will cause harm. Women with large breasts or with breast implants may be exposed to slightly higher radiation doses during screening mammography.
There may be pain or x-ray discomfort during a mammogram.
During a mammogram, the breast is placed between two plates that are pressed together. Pressing the breast helps to get a better of the breast. Some women have pain or discomfort during a mammogram. The amount of pain may also depend on the following:
- The phase of the woman's menstrual cycle.
- The woman's anxiety level.
- How much pain the woman expected.
Talk to your doctor about your risk of breast cancer and your need for screening tests.
Talk to your doctor or other care provider about your risk of breast cancer, whether a screening test is right for you, and the benefits and harms of the screening test. You should take part in the decision about whether you want to have a screening test, based on what is best for you. For more information, see Cancer Screening Overview.
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about breast cancer screening. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Screening and Prevention Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Screening and Prevention Editorial Board. PDQ Breast Cancer Screening. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/breast/patient/breast-screening-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389160]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2023-06-26
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.

